What is RehaMove?
A neurological disease often leads to nerve damage. The muscles supplied by the paralyzed nerve no longer receive any impulses. The result: muscle cells break down. With RehaMove, impulses can be generated and muscles can be stimulated.


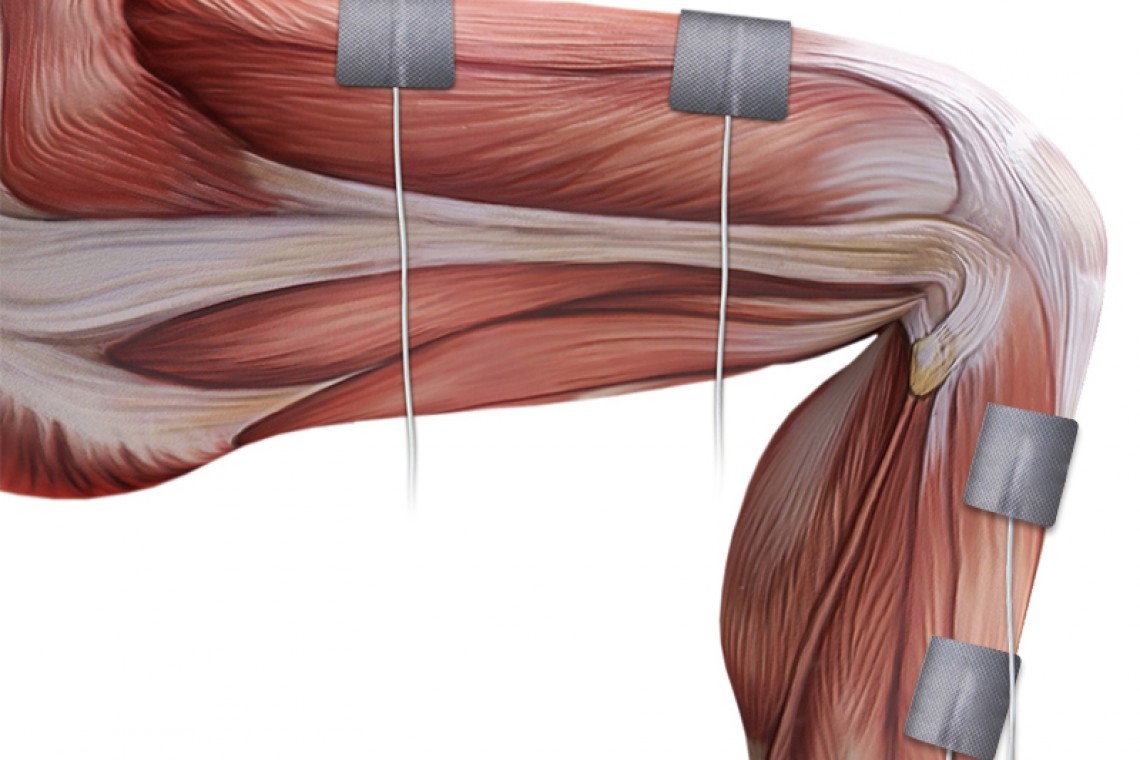
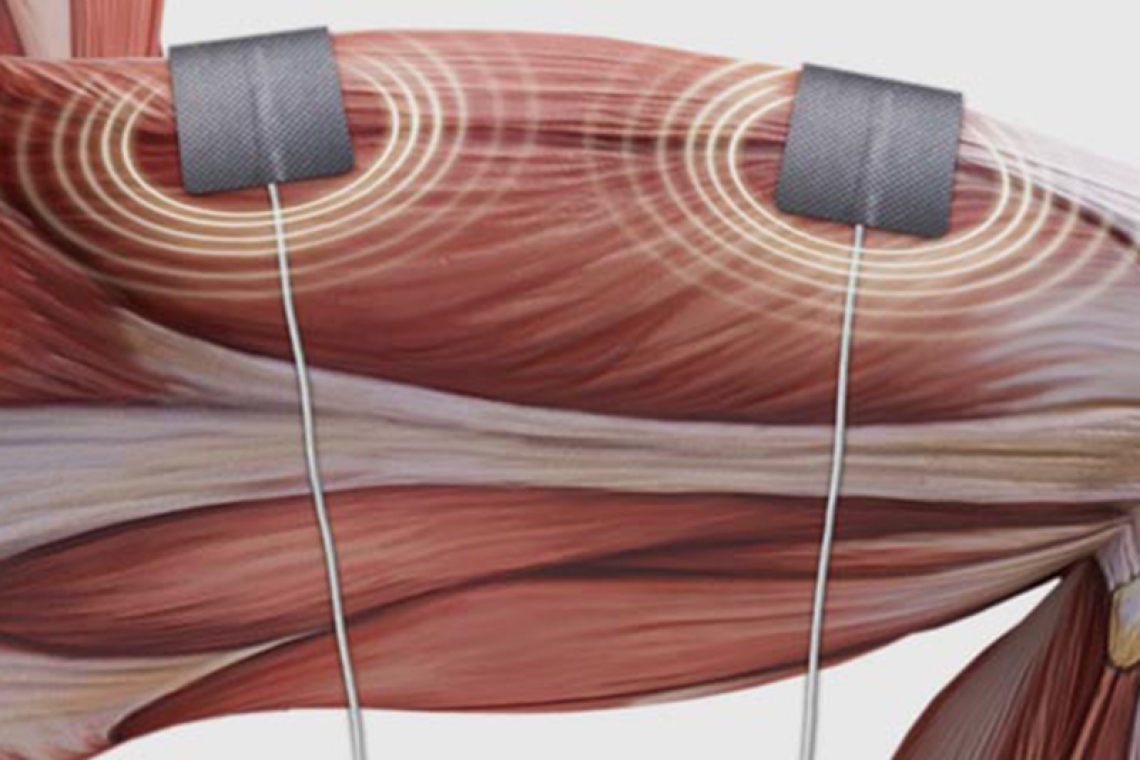




Functional electrical stimulation (FES) is a therapy method where nerves are stimulated with electrical current via surface electrodes in order to cause muscular contraction. The aim is to produce a functional movement for impaired extremities. With RehaMove, specific movement sequences can be generated - for example during cycling, gait training, stabilization exercises or for foot dorsiflexion.
FES-assisted movement training with RehaMove is very important during therapy and rehabilitation processes of paralyzes. It is an effective method to relieve muscle spasms, prevent or avoid atrophy due to immobilization, increase the local blood flow or increase respectively maintain the range of motion. Therapy with functional electrical stimulation is for example recommended in Germany and part of the evidence-based S2 guideline "Rehabilitation of the lower extremities, standing and walking function in people with paraplegia".
What does RehaMove do?
FES-assisted movement training with RehaMove is very important during therapy and rehabilitation processes of paralyzes. It is an effective method to relieve muscle spasms, prevent or avoid atrophy due to immobilization, increase the local blood flow or increase respectively maintain the range of motion. Therapy with functional electrical stimulation is for example recommended in Germany and part of the evidence-based S2 guideline "Rehabilitation of the lower extremities, standing and walking function in people with paraplegia".

Early rehabiliation
In the early rehabilitation of neurological patients, safety and active stimulation are crucial for therapeutic success. The ErigoPro combines the gradual verticalization with the cyclical movement and loading of the legs and thus provides the necessary safety to stabilize the patient in an upright position. In combination with RehaMove, positive effects, for example increased local blood flow can be achieved.

FES-Cycling
Active movement is a prerequisite for health and wellbeing. The MOTOmed movement trainer can be combined with RehaMove. RehaMove stimulates the muscles so that legs and/or arms move with their own strength. This turns passive movement into active movement training.

FES-Walking
FES Walking can effectively mobilize people with incomplete paraplegia and prepare them for gait training. In hemiplegic patients, the paralyzed leg can be supported at the push of a button (external trigger) and strength deficits can be compensated.
Sequence Training
With sequence training, applications from 1-channel hand extension to 8-channel gait training are possible. Standardized application templates allow to stimulate movement sequences extremily fast and without further efforts. Each sequence training can be adapted with individual adjustable stimulation and pause times. The stimulation can be triggered automatically or manually. The manual starting and stopping of stimulation sequences can be done directly via the stimulator or via a manual switch - external trigger. One focus of this application is gait training: for hemiplegic people, the paralyzed leg can be supported and strength deficits are compensatedwith the support of the external trigger. People with incomplete paraplegia can be mobilized more effectively and prepared for gait training.
Do you already know the newsletter of HASOMED GmbH? Here you will receive all information about updates, product enhancements as well as current offers and dates.
How can I get to know RehaMove?
Medica 2019: Innovative HASOMED medical devices at the World Forum of Medicine
The UN forecasts a world population of more than 9.7 billion people by 2050. A challenge for medical care and a task that physicians and manufacturers of medical technology can master together. Medica 2019, World Forum of Medicine, creates the link between medicine and medical technology, present and future. HASOMED is there.